Valley Fever and Areas of Risk
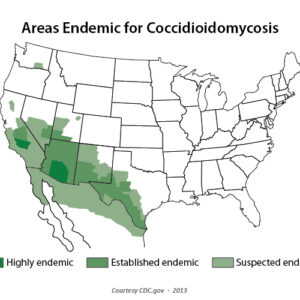
Valley fever, also called coccidioidomycosis, is an infection caused by the soil-dwelling fungus Coccidioides. The fungus is commonly found in the arid soil in the southwestern US and parts of Central and South America, as it is dependent on both weather patterns and soil composition for growth. It has also recently been found in south-central Washington. Humans and animals contract the infection by breathing the fungal spores from the air, often after disturbance of contaminated soil. In the US, highly endemic areas include southern Arizona and California’s southern San Joaquin Valley. Notably in Washington, 12 human cases with suspected exposure in Washington have been reported since 2010, all from south-central Washington.
Although most people who breathe in the spores do not get sick, certain groups are at higher risk for becoming severely ill, such as those who have weakened immune systems, pregnant women, people with diabetes, and African-Americans and Filipinos. Most infections are sub-clinical with no symptoms or mild flu-like symptoms. Symptomatic persons, representing approximately 40% of cases, usually present 1-3 weeks after exposure with fatigue, cough, dyspnea, headache, night sweats, myalgias, and rash. Primary pulmonary disease is often self-limiting, but some patients fail to recover and develop complications or chronic pulmonary disease (5-10% of cases). Disseminated disease occurs in an estimated 1% of cases.
Serologic tests to detect IgM and IgG antibodies are most often used for diagnosis. IgM antibodies are detectable in about 50% of patients by one week after symptom onset and about 90% by three weeks. IgG antibodies are generally detectable by 4-6 weeks, and 85-90% of patients have detectable IgG by three months. All serology is generally considered acute testing and a marker for current or recent infection. Other methods include using culture and microscopy. Culture can be performed on tissue and respiratory specimens, although sputum can be difficult to obtain for culture since patients’ coughs are often non-productive.